Table of Contents
- INTRODUCTION:
- RECTUM : Anatomy
- Extent:
- Course and Direction :
- Relations :
- Interior of Rectum :
- Arterial supply :
- Venous supply :
- Lymphatic drainage :
- Nerve Supply :
- Supports of the Rectum :
- Examination of the rectum :
- Rectal diseases and abnormalities :
- Congenital [ Present from the birth ]
- Structural abnormalities
- Common benign conditions
- Inflammatory diseases
- Benign tumors and polyps
- Precancerous conditions
- Cancerous diseases
- Vascular disorders
- Fistulas and abscesses
- Functional disorders
- Common symptoms of rectal disorders
- Conclusion :
- References
INTRODUCTION:
Rectum and anal canal are the distal ends of the gastrointestinal tract respectively . After digestion of food , nutrients get absorbed from the GIT and supplied to the whole body. The remaining wastes which are formed at the end of digestion are turned into faeces and get stored in rectum for sometime and thrown out from the body through anal canal.
RECTUM : Anatomy
Rectum is the distal part of large intestine present in between the sigmoid colon and the anal canal . It is curved anterio-posteriorly and also side to side . Rectum stores the faecal matter for some time . Distension of the rectum causes desire to defecate .
Note : Three cardinal featuers that are present in the large intestine and absent in the rectum
- Sacculations
- Taenia
- appendices epiploicae
Location : Located in front of the lower three pieces of the sacrum [S3,S4,S5] and the coccyx . Posterior part of lesser pelvis.
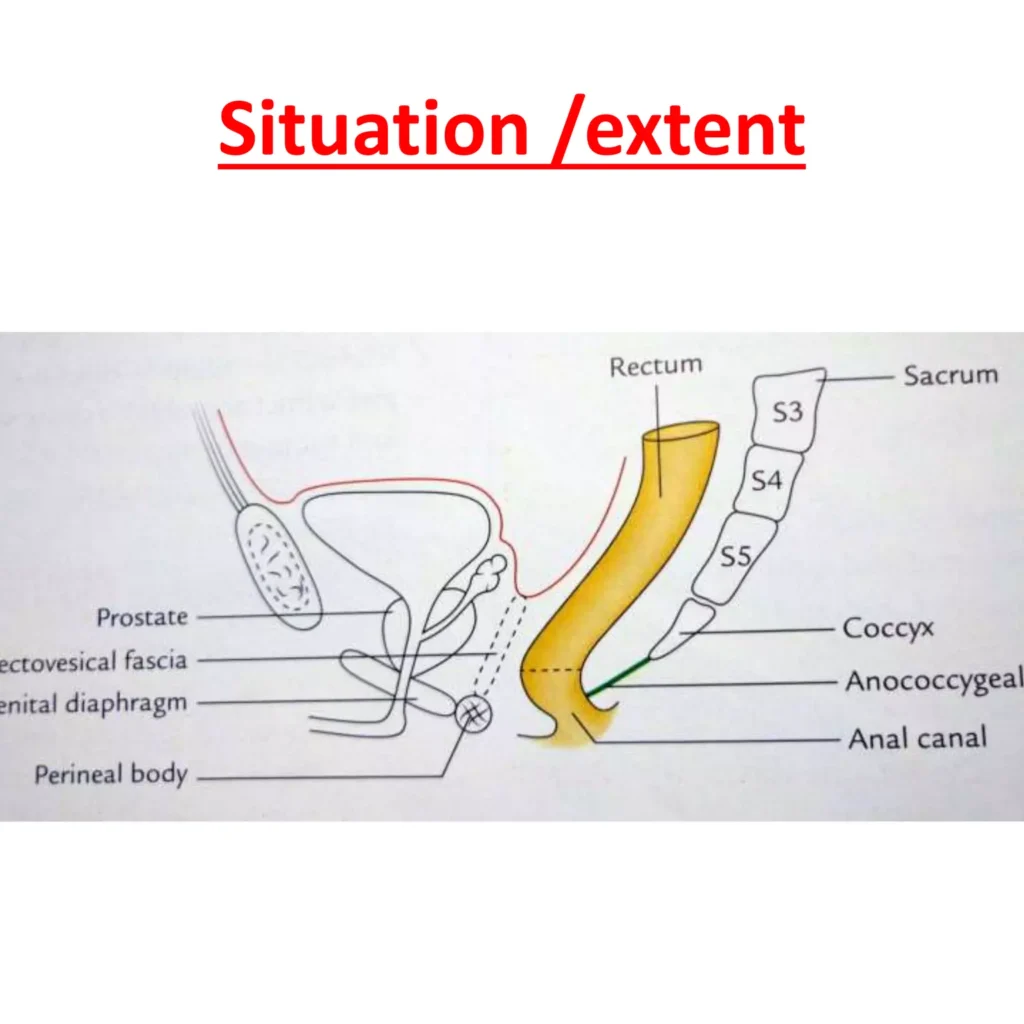
Extent:
- Rectum begins as continuation of sigmoid colon at the level of S3 vertebrae .
- It starts at the rectosigmoidal junction indicated by the lower end of the sigmoid mesocolon.
- It ends at the anorectal junction , this junction lies in 2 to 3 cm in front of and a little below the tip of coccyx .
- In males junction corresponds to the apex of the postrate.
- In females lower quater of vagina .
- DIMENSIONS : It is 12 cm long [5 inch ]
- Upper part has the same diameter of sigmoid colon that is of 4 cm .
- Lower part is dilated to form the rectal ampulla .
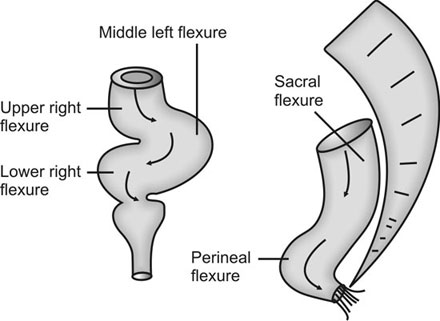
Course and Direction :
- Firstly it runs downward and backward , then downward , finally downward and forward.
- The beginning and the ending of the rectum lies in the medial plane .
- But it shows 2 types of curvatures in anterioposteriorly
- Sacral flexure – Follows concavity of the sacrum and the coccyx
- perineal flexure – Acute posterior bend at the level of the anorectal junction where puborectalis forms a sling that pulls the bowel forward .
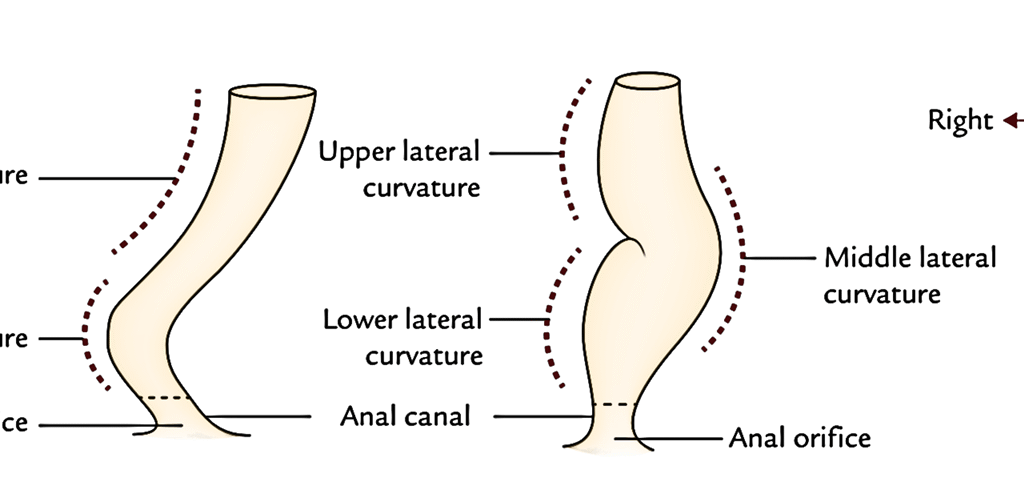
- 3 Lateral curvatures :
- Upper lateral curve : Convex to the right
- Middle lateral curve : This is most prominent and convex to the left .
- Lower lateral curve : Convex to the right.
Relations :
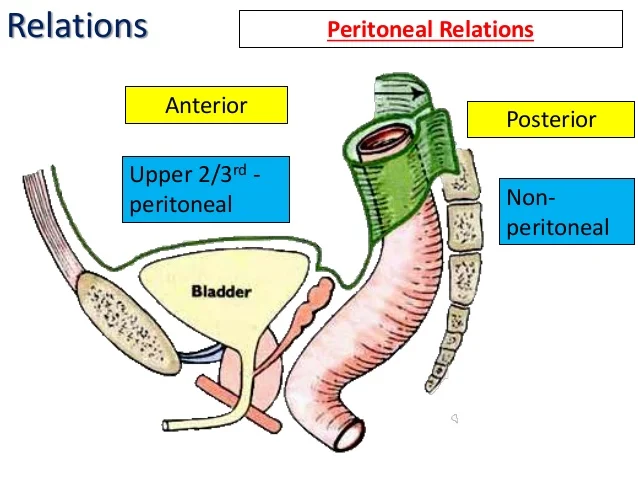
PERITONEAL RELATIONS :
- UPPER 1/3rd – Covered with peritoneum in front and on the sides
- Middle 1/3rd – Covered only in front .
- Lower 1/3rd – It dilates and form the ampulla and it is devoid of peritoneum .
- Males- lies below the recto vesical pouch and the distance between the anus and the floor of the pouch is 7cm .
- Females -lies below the rectouterine pouch and the distance between the anus and the floor of the pouch is 5.5 cm .
VISCERAL RELATIONS:
- Posterior relations : Same in males and females
- lower 3 pieces of sacrum [S3,S4,S5] Coccyx and the anococcygeal ligament
- Muscles – pyriformis, coccygeus and levator ani
- Vessels – median sacral , superior rectal ,lower lateral sacral vessels
- Nerves – Sympathetic chain with the ganglion impar ,the anterior primary rami of S3 S4 S5 coccygeal 1 and the pelvic splanchnic nerves ,lymph nodes , lymphatics and fat.
- Anterior relations :
- Males :
- Upper 2/3rd of rectum – Rectovesical pouch with coils of intestine and sigmoid colon .
- Lower 1/3rd of rectum
- Base of the urinary bladder
- the terminal part of the ureters
- the seminal vesicles
- the ductus deferens and the prostate .
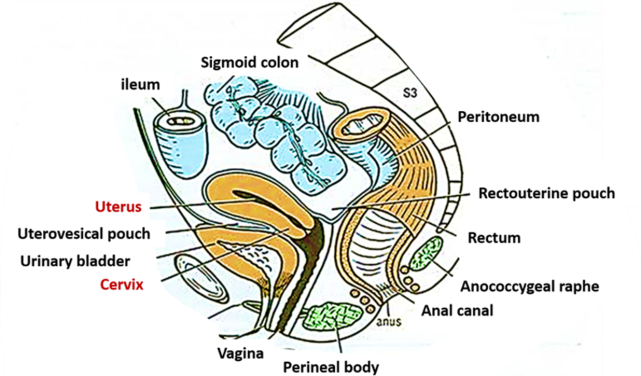
- Females :
- Upper 2/3rd of rectum – Rectouterine pouch with coils of intestine and sigmoid colon .
- Note : this rectouterine pouch separates the rectum from uterus and form the upper part of the vagina .
- Lower 2/3rd of rectum -Lower part of the vagina .
- Upper 2/3rd of rectum – Rectouterine pouch with coils of intestine and sigmoid colon .
- Males :
Interior of Rectum :
Mucous membrane of an empty rectum shows two types of folds .
- Longitudinal
- Transverse
Longitudinal folds : These are transitory[temporary] . They are present in the lower part of an empty rectum , obliterated by distension .
Transverse folds :
- These folds are also called as Horizontal folds or Houston’s valves or plicae transversales .
- These are permanent and most marked when rectum is distended .
- First transverse fold
- Lies near the upper end of the rectum .
- projects from the left wall situated about 15cm above anus .
- Sometimes , it may encircle and partially constrict the lumen
- Second transverse fold
- This large and most constant.
- lies in upper end of the rectal ampulla about 8cm from anus .
- It projects from the anterior and the right walls
- Third transverse fold
- It is inconstant lies 2.5cm below the second fold, and projects from the left wall.
- First transverse fold
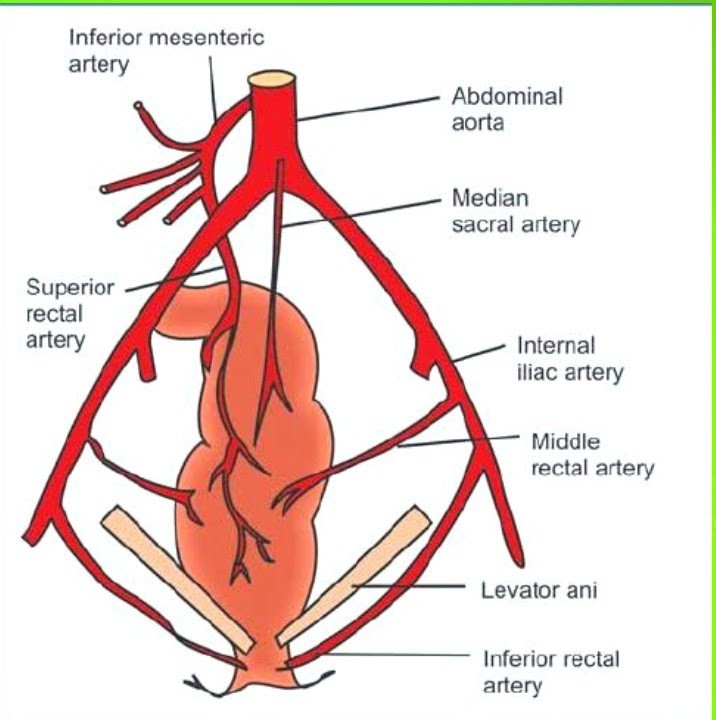
Arterial supply :
- Superior rectal artery :
- This is chief artery of rectum
- It is continuation of inferior mesenteric artery.
- Middle rectal arteries :
- arise – Anterior division of the internal iliac artery and run in lateral ligaments of rectum
- supply – only superficial muscle coats of lower part of the rectum .
- anastomoses of these arteries are poor.
- Median sacral artery :
- small branch arising from the back of the aorta near its lower end .
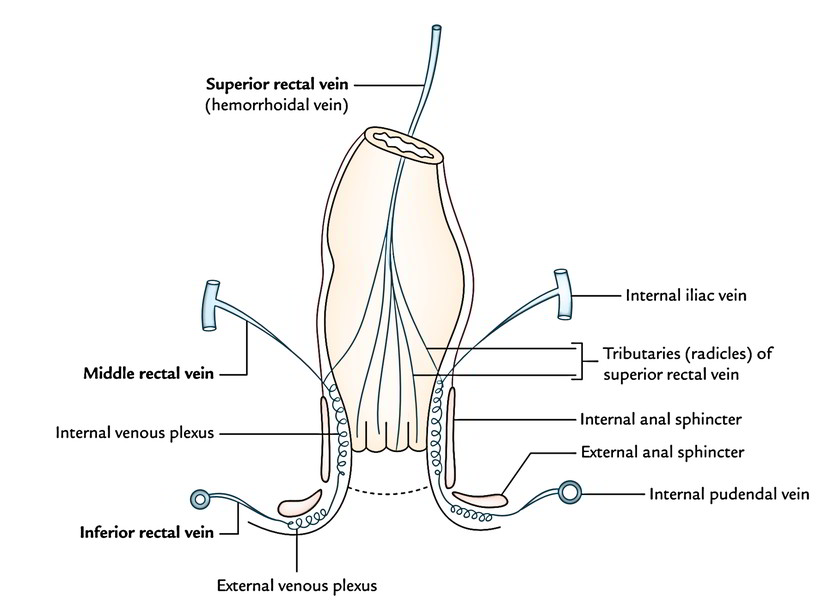
Venous supply :
- Superior rectal vein :
- Internal rectal venous plexus – Tributaries of this vein begin in anal canal [ in form of three veins ] – passes upward in rectal submucosa ,and pierce the muscular coat about 7.5 cm above the anus – unite to form the superior rectal vein – continue upwards as the inferior mesenteric vein – end in splenic vein .
- Middle rectal vein :
- Tributaries of this vein drain chiefly , into the muscular walls of rectal ampulla and open into the internal iliac veins .
- Median sacral vein :
- it joins left common iliac vein .
Lymphatic drainage :
- Upper half of the rectum : pass along the superior rectal vessels to pararectal and sigmoid nodes and then to inferior mesenteric nodes .
- Lower half of the rectum : along middle rectal vessels to the iliac nodes .
Nerve Supply :
- It is supplied by both sympathetic and the parasympathetic nerves through the superior rectal or inferior mesenteric and inferior hypogastric plexuses .
- Sympathetic – [L1,L2] These nerves are vasoconstrictors.
- Inhibitory to the rectal musculature .
- Motor to the internal sphincter .
- Parasympathetic – [S2,S3,S4] – Sensation of distension of the rectum.
- Motor to the rectal musculature.
- Inhibitory to the internal sphincter .
- Pain sensation is carried by both the sympathetic and parasympathetic nerves .
- Sympathetic – [L1,L2] These nerves are vasoconstrictors.
Supports of the Rectum :
- Pelvic floor formed by levator ani muscles
- Fascia of Waldeyer : It attaches the lower part of rectal ampulla to the Sacrum
- Formed by condensation of the pelvic fascia behind the rectum .
- It encloses the superior rectal vessels and lymphatics.
- Lateral ligaments of the rectum – It attaches the posterior lateral walls of rectum to the lesser pelvis .
- formed by condensation of the pelvic fascia on each side of the rectum .
- It encloses the middle rectal vessels and branches of the pelvic plexuses .
- Rectovesical fascia of Denonvilliers : Extend from the rectum behind to the seminal vesicles and prostrate in front .
- Pelvic peritoneum and related vascular pedicles .
- perineal body with its muscles .
Examination of the rectum :
- Examination of rectum is done by the following procedures:
- Digital rectal examination (DRE) – A healthcare provider inserts a gloved, lubricated finger into the rectum to feel abnormalities.
- Anoscope -Uses a short, rigid tube (anoscope) to examine the anal canal and lower rectum.
- Proctoscope – Uses a proctoscope to examine the rectum and anal canal.
- Rigid sigmoidoscopy – Uses a rigid instrument to examine the rectum and lower sigmoid colon.
- Flexible sigmoidoscopy – Uses a flexible endoscope to examine the rectum and sigmoid colon.
- Colonoscopy – Uses a flexible endoscope to examine the rectum, the entire colon .
Rectal diseases and abnormalities :
Congenital [ Present from the birth ]
- Imperforate anus
- Rectal atresia
- Rectal stenosis
- Rectal duplication cyst
- Persistent cloaca
- Rectourethral fistula
- Rectovaginal fistula
Structural abnormalities
- Rectocele
- Rectal prolapse
- Internal rectal prolapse
- Rectal intussusception
- Solitary rectal ulcer syndrome
- Descending perineum syndrome
Common benign conditions
- Hemorrhoids
- Anal fissure
- Rectal ulcer
- Mucosal prolapse syndrome
Inflammatory diseases
- Ulcerative colitis
- Crohn’s disease
- Proctitis
- Radiation proctitis
- Diversion proctitis
- Ischemic proctitis
- Eosinophilic proctitis
Benign tumors and polyps
- Hyperplastic polyp
- Adenomatous polyp
- Sessile serrated lesion
- Inflammatory polyp
- Hamartomatous polyp
- Rectal lipoma
Precancerous conditions
- Rectal adenoma
- High-grade dysplasia
Cancerous diseases
- Rectal cancer
- Squamous cell carcinoma of the rectum
- Gastrointestinal stromal tumor
- Lymphoma
- Melanoma
- Metastatic cancer to the rectum
Vascular disorders
- Rectal varices
- Angiodysplasia
- Rectal bleeding due to vascular ectasia
Fistulas and abscesses
- Perirectal abscess
- Rectal fistula
- Rectovaginal fistula
- Rectovesical fistula
- Rectourethral fistula
Functional disorders
- Dyssynergic defecation
- Rectal hyposensitivity
- Fecal incontinence
- Obstructed defecation syndrome
- Chronic constipation
Common symptoms of rectal disorders
Many of these conditions can cause:
- Rectal pain
- Bleeding from the rectum
- Blood in stool
- Mucus discharge
- Constipation
- Diarrhea
- A feeling of incomplete emptying
- Rectal pressure
- A lump or prolapse
- Fecal leakage
- Unexplained weight loss (more concerning)
Conclusion :
The rectum is an essential part of the digestive system, serving as the temporary storage site for feces before elimination. Its structure and function play a vital role in maintaining normal bowel movements and overall digestive health. Understanding the anatomy, physiology, and common disorders of the rectum can help promote early diagnosis, effective treatment, and preventive care. Maintaining a healthy diet, staying physically active, and seeking timely medical attention for persistent symptoms are important steps in preserving rectal health and improving overall well-being.
References
- Gray’s Anatomy: The Anatomical Basis of Clinical Practice.
- B.D. Chaurasia’s Human Anatomy, Volume 2.
- Clinically Oriented Anatomy by Moore, Dalley & Agur.
- Last’s Anatomy.
- Snell’s Clinical Anatomy.
- Cunningham’s Manual of Practical Anatomy.
- Kenhub – Rectum Anatomy.
- TeachMeAnatomy – Rectum.
- Standard colorectal surgery or gastroenterology guidelines where clinical recommendations are discussed.
- https://www.innerbody.com/image_digeov/dige14-new3.html